a segment of the left pulmonary artery resected for 7 cm and the anterior wall of the pulmonary artery trunk (Fig. 74). The lung has expanded, the artery is pulsating well. Antibiotics and two drainages into the pleural cavity. Sutures on the chest wall wound.
Bronchoscopy: in the area of the anastomosis there is good adaptation of the edges of the mucous membrane, the lumen of the anastomosis is not narrowed.
Macroscopic specimen: the lobe is dense, with fragments of adhesions. At the root there are dense lymph nodes measuring up to 5X3 cm. The lung tissue is
Rice. 75. The same patient. Angiopulmonogram 1"/a month after surgery. The vessels of the remaining lobe of the left lung are well contrasted.
gray-red section. In the 1st segment, the dilated bronchi are filled with mucopurulent masses. The lines of intersection of the bronchus are located at a distance of 3 and 1.5 cm from the edge of the tumor. The mucous membrane of the resected sections of the main and lower lobe bronchi is unchanged. On the section, the lumen of the upper lobe bronchus is obstructed by a dense tumor, partially protruding into the lumen of the main bronchus. The tumor forms an irregularly shaped node measuring 3.5x2x2.5 cm, which grows into the lobar bronchus and spreads into the lung tissue. The pulmonary artery is intimately fused with the tumor for 1 cm.
Histological examination of the specimen: undifferentiated small cell carcinoma. In the lymph nodes there are massive metastases of cancer of the same structure. No tumor elements were found in the sectional edge of the bronchus. In the lung tissue, fibroatlectasis, retention bronchiectasis, chronic interstitial pneumonia.
The postoperative period was complicated by atelectasis of the lobe on the side of the operation. Therapeutic bronchoscopy with aspiration was used
viscous sputum. Otherwise, the postoperative course was uneventful.
1"/2 months after the operation, the bronchial anastomosis is in good condition. During angiopulmonography, the vessels of the lower lobe of the left lung are well contrasted (Fig. 75).
The main contraindication to lobectomy and bronchoplasty for upper lobe bronchopulmonary cancer is the high prevalence of the process. In each specific case, contraindications to bronchoplasty should be assessed individually. We narrow them somewhat during operations on elderly people with low functional reserves, especially with right-sided cancer. In this category of patients, a “compromise” lobectomy with resection and bronchoplasty is often preferable to a more life-threatening and usually disabling pulmovectomy.
OTHER INDICATIONS
The need for resection and plastic surgery may arise with inflammatory narrowing of the bronchi, polypous endobronchitis and suppurating bronchogenic cysts of the hilar localization.
Narrowing of the bronchi due to a nonspecific inflammatory process is rare. Narkiewicz et al. (1964) described 3 patients operated on for nonspecific limited endobronchitis. The differential diagnosis should take into account syphilis, bronchopulmonary tumors, tuberculosis and bronchial foreign bodies.
The extent of surgical intervention for inflammatory stenosis depends on the degree of changes and the condition of the pulmonary parenchyma. Sometimes it is enough to remove granulation tissue from the bronchial lumen or excise scar peribronchial cords. For limited lesions, segmental or wedge resection of the bronchus is indicated.
We observed 2 patients with chronic suppuration of the upper lobe of the right lung and narrowing of the lobar bronchus caused by a nonspecific inflammatory process. In one patient, chronic nonspecific pneumonia with bronchiectasis was a consequence of polypous endobronchitis of the middle lobe bronchus. These 3 patients underwent lobe removal with wedge-shaped resection of the main bronchus.
In one case, indications for resection of the right main bronchus arose due to a suppurating bronchogenic cyst of the upper lobe. A typical lobectomy could not be performed, since the thickened wall of the cyst was tightly fused with the lobar and main bronchi. The upper lobe was removed with a wedge-shaped resection of the main bronchus.
CHAPTER I V
METHODS AND TECHNIQUES OF OPERATIONS
ANESTHESIA
All plastic surgeries on large bronchi must be performed under anesthesia with controlled breathing.
The main feature of anesthesia during resection and plasty of bronchi is the need to ensure sufficient pulmonary ventilation during prolonged gaping of the lumen of the trachea or crossed large bronchus (T. T. Bogdan, 1955;
IN. S. Severov, 10. N. Zhilin, A. P. Davydov, 1961; F. F. Amirov, 1962; O. M. Avilova, E. P. Kravchenko, 1964; L.K. Bogush,
IN. S. Severov, Yu. N. Zhilin, V. F. Didenko, 1965; O. D. Kolyutskaya, V. S. Trusov, V. N. Tsibulyak, 1965, etc.). It should also be borne in mind that plastic surgery on the bronchi is often performed in elderly patients with significant changes in the respiratory and cardiovascular system and low functional reserves.
Before the operation, the anesthesiologist must familiarize himself in detail with the nature of the pathological process based on radiological and bronchological data, and then discuss with the surgeon the plan for the upcoming intervention and possible options for resection and reconstruction of the tracheobronchial tree.
In the operating room it is necessary to have a set of sterile endotracheal tubes for various methods of endotracheal and endobronchial intubation, as well as sequential reintubation during anesthesia. If there is a likely need for trial inflation of an atelectatic lung after bronchial rupture, a second anesthesia machine with sterile endotracheal and connecting tubes should be prepared.
8 Order 255 |
They are also needed for intubation of the crossed bronchus from the side of the pleural cavity in cases of possible need for resection of the tracheal bifurcation.
During the examination and preparation for surgery, patients with concomitant diseases are prescribed the necessary therapy. We prescribed Andaxin or Mekraton 200 mg 2-3 times a day to excited patients with a labile psyche 2-3 days before surgery. Glucocorticoids, as a rule, were not prescribed due to their possible negative effect on the regeneration process.
Anesthesia was administered according to the following method:
200 mg promedol and 1 mg atropine. Induction of anesthesia is carried out by inhalation of fluorotape with nitrous oxide and oxygen through a mask with simultaneous intravenous injection of barbiturates or steroid drugs. Depolarizing muscle relaxants are used for intubation.
In order to ensure adequate ventilation of the lungs during a wide opening of the trachea and bronchi, various techniques can be used. In an experiment on animals, we compared the effectiveness of a number of them. The transected bronchus was closed with a clamp or gauze pad from the side of the wound, bronchial blockers, endobronchial intubation with single-lumen and double-lumen tubes, transpleural intubation with switching off one lung and shunt breathing were used. As a result of experimental studies and mainly clinical experience, we consider endobronchial intubation to be the most rational method for all plastic surgeries on the bronchi. This method allows for complete ventilation of a healthy lung after crossing the bronchus on the side of the operation, and prevents the flow of sputum, pus and blood into the ventilated lung.
Prevents obstruction of the airways with pieces of tissue or tumor and creates optimal conditions for the operating surgeon.
In clinical practice during operations on the right main
bronchus, either a conventional single-lumen tube or a Gordon-Green tube must be inserted into the right bronchus. Even more convenient
an inflatable cuff (Fig. 76). This tube was manufactured at the Institute

Rice. 76. Double-lumen tube with a narrow inflatable cuff.
A - tube design diagram; B - guide for intubation; B - position of the tube in the right and left bronchi.
tut rubber and latex products and has been successfully used in more than 40 different operations on the lungs and bronchi.
The choice of intubation method depends not only on the side of the lesion, but also on the characteristics of the pathological process and the nature of the surgical intervention. Therefore, during the operation it is sometimes necessary to reintubate the patient.
A schematic representation of the main options for intubation during typical plastic surgeries on large bronchi is presented in Fig. 77.
Ether, ether with nitrous oxide, fluorotane, fluorothane with nitrous oxide, chloroform or trilene with nitrous oxide can be used as the main narcotic substances. Their application on our material is shown in Table. 18.
TABLE 18 |
||||||||||
Application |
various main |
narcotic |
||||||||
plastic |
operations |
on the bronchi |
||||||||
Post-traumatic |
||||||||||
occlusion |
||||||||||
Tuberculosis |
||||||||||
bronchus infection |
||||||||||
Posttuberculosis |
||||||||||
bronchoconstriction |
||||||||||
Good quality |
||||||||||
bronchial tumors |
||||||||||
And so on. . . |
||||||||||
Recently, our anesthesiologists have been using fluorotane or chloroform as the main narcotic substances during plastic surgery on the bronchi. These anesthetics have significant advantages over ether and nitrous oxide. A gas-narcotic mixture with fluorotane or chloroform has strong narcotic properties, does not irritate the mucous membrane of the respiratory tract, is explosion-proof and allows you to create any concentration of oxygen, which is especially important during long-term removal of one lung from ventilation.

Rice. 77. Scheme of the main options for intubation during plastic surgery on large bronchi.
Fluorotane and chloroform are used according to the generally accepted method through a “fluorotek” designed by VNIIMIiO or a “fluotek Mark-P” placed outside the gas circulation unit.
When maintaining basic anesthesia along a semi-closed circuit, the concentration of the drug in the inhaled mixture does not exceed 1.5 vol.% with an oxygen flow of up to 5 L / M. The method of choice can be considered maintaining anesthesia with a gas-narcotic mixture consisting of 0.5 vol. % fluorothane in a flow of nitrous oxide with oxygen in a ratio of 2:1, 1:1.
Artificial ventilation of the lungs is carried out using an automatic respirator AND-2 against the background of prolonged apnea caused by the administration of antidepolarizing type muscle relaxants, in
mode of moderate hyperventilation |
not lower than 28 mm |
||
From the main bronchus of the operated side |
through a catheter, |
||
entered into the appropriate channel |
intubation |
||
ki, constantly or periodically suction |
|||
In cases of prolonged shutdown |
from ventilation |
||
If the lung becomes airy, so-called splenization may develop. It occurs due to the sweating of fluid and even blood cells from the pulmonary capillaries into the alveoli. In order to prevent splenization, switching off the lung from ventilation on the operated side should be done only after separation of all pleural adhesions. This technique also makes it possible to prevent hypoxia due to the large discharge of unoxygenated blood into the left atrium. After complete collapse of the lung, the blood flow in it sharply decreases and the arteriovenous shunt is less pronounced.
During the period of bronchial anastomosis, it is advisable to ventilate the lung not automatically, but manually, in accordance with the surgeon’s manipulations and facilitating them as much as possible.
The significant duration of the surgical intervention and the complexity of pain relief at some stages necessitate constant electrocardiographic and encephalographic monitoring. In the most severe patients, it is also necessary to examine the acid-base state and the volume of circulating blood.
After suturing the chest wall wound, a bronchoscopic examination is performed to control the anastomosis and thoroughly clean the bronchial tree. The tube of the respiratory bronchoscope is removed after removal of residual curarization and restoration of adequate spontaneous breathing.
An example of the course of anesthesia during lobectomy with resection of the main bronchus is shown in Fig. 78.

Rice. 78. Patient K., 55 years old. Upper lobectomy on the right with circular resection of the main bronchus. The main anesthesia is chloroform in a stream of nitrous oxide.
Anesthesiologist card. One-lung ventilation 3 hours 10 minutes.
The need for shunt breathing, which is carried out through an endotracheal tube inserted into the peripheral end of the transected bronchus from the side of the opened pleural cavity, did not arise in our material.
There were no complications associated with anesthesia during anesthesia and in the early postoperative period.
ONLINE ACCESS
Most plastic surgeries on the bronchi are combined with various options for lung resection. Sometimes, during the course of the intervention, there is also a need for marginal or circular resection of the pulmonary artery with the application of a side suture or interarterial anastomosis end to end or side to end. Therefore, the approach used should ensure that pulmonary surgery is performed with a sufficiently free field for manipulation in the area of the tracheobronchial angle, the division of the main bronchi and the location of large pulmonary vessels. The listed requirements are most satisfied by a standard lateral thoracotomy along the fifth intercostal space with the patient positioned on the healthy side.
Standard lateral thoracotomy makes it possible to freely perform the necessary manipulations in all parts of the pleural cavity, provides a convenient approach to the tracheobronchial angle, to all elements of the lung root and to the main interlobar fissure. With this access, there is full possibility of plastic surgery on the bronchi and lower trachea with simultaneous removal of the affected part of the lung. It is also possible to combine reconstructive surgery on the bronchi with marginal or circular resection of the pulmonary artery.
In some patients, however, it is better to use a posterior approach rather than a lateral one in the prone position with opening of the hymen
We consider reconstructive surgery after a traumatic bronchial rupture to be a direct indication for the posterior approach. Experience shows that in these cases, the posterior separation of the main bronchus from the scar tissue of the mediastinum is significantly facilitated and the risk of damage to the great vessels of the collapsed lung is reduced.
The second direct indication for the posterior approach is surgery for a benign tumor, which is localized at the mouth of the main bronchus. At the same time, there is always
Or rather, its tactics directly depend on the degree of development of the oncological process, its form, the presence of metastasis to nearby organs and tissues, and the effectiveness of histological tests. In 80% of cancer patients, radical intervention has proven its effectiveness; in more than 30% of patients with lymph nodes affected, surgery prolongs life.
How is surgery performed for bronchial cancer?
Depending on the indications, treatment is carried out as follows: Removal of part of the lung: lobectomy - resection of one lobe of the organ, bilobectomy - excision of two lobes of the lung; Complete resection of the lung: pneumonectomy, pneumonectomy with mediastinal lymphadenectomy, excision of a segment of the trachea in the area of its division into the main branches with restoration of the integrity of the tracheobronchial tree, pneumonectomy with circular resection of the superior vena cava/thoracic aorta. In some cases, when a cancerous process is detected in the early stages, a circular or fenestrated removal of the organ is performed. To combat the oncological process, surgical or combined methods are used. Combined includes the use of gamma therapy. The cost of surgery for bronchial cancer using gamma therapy depends on the course of the pathological process, its stages. Cancer, as a rule, metastasizes to nearby lymph nodes in a short time, so any intervention involves excision of those lymph nodes that receive lymph from the affected organ. This approach to treatment minimizes the risk of possible progression of the pathology and relapses, which significantly increases the life expectancy of patients. The intervention begins with opening the chest (thoracotomy), followed by fixation of the vessels, cauterization and suturing. After this, the surgeon removes the required section of the lung, or performs a complete resection of the organ, fatty tissue and lymph nodes, and then creates a stump. The cavity part in which the lung was located undergoes restoration and reduction. At the end of the procedure, drainage is installed and sutures are applied. The patient is transferred to the intensive care unit, where artificial ventilation (ALV) will be used until the person emerges from anesthesia.
How much does surgery to remove bronchial cancer cost?
In various Moscow clinics, the cost of surgery to remove bronchial cancer is determined on an individual basis. The cost includes diagnostic measures, the extent of surgical intervention, and the duration of the postoperative period. You can make an appointment with a qualified specialist or fill out an application for surgical treatment on our website.
Postoperative period for bronchial cancer
Rehabilitation after surgery for bronchial cancer involves careful monitoring of the patient’s condition, blood pressure control, respiratory function. In the first few days, active aspiration of the pleural cavity is carried out using drainage and suction. The patient is prescribed a course of antibiotic therapy and other medications, depending on the outcome of the intervention and possible adverse consequences. Gentle dietary nutrition is necessary in the first two to three days. The patient is taught special breathing exercises, which improve blood circulation and prevent congestion in the lungs and bronchi. Consequences after surgery for bronchial cancer can manifest themselves in the form of relapses of oncological processes in the remaining part of the organ, but only if there is infiltration of the bronchial wall behind the visible outlines of the tumor formation.
4278 0
Indications for endoscopic operations are tumors and cicatricial stenoses of the trachea and large bronchi. This provision needs clarification. First of all, pathological changes must be accessible to a rigid bronchoscope, i.e., localized in the trachea, main, intermediate and lobar bronchi. With a deeper tumor location, surgery is possible in some cases, but requires the use of a bronchofiberscope and is associated with certain technical difficulties.
Endoscopic operations on the trachea and bronchi should in no case be opposed to classical open operations, the possibilities and radicality of which are immeasurably higher. However, due to significantly less trauma, endotracheal and endobronchial operations have advantages in the following specific situations.
Endoscopic operations are indicated for exophytically growing benign tumors of the trachea and large bronchi, when their removal using an electrocoagulation loop or laser is quite radical. This primarily applies to single papillomas, in which recovery usually occurs after technically correct removal. Quite rare endobronchial polyps and tumors of non-epithelial origin can be radically removed endoscopically: fibromas, lipomas, fibrolipomas, etc.
For multiple papillomas of the larynx, trachea and large bronchi, which are prone to relapse, endoscopic operations, although not radical, can be considered the method of choice, since classical open operations are usually contraindicated.
Endoscopic operations can be performed for relatively rare so-called typical carcinoids of the trachea and large bronchi that grow exophytically and have a well-formed stalk. With combined (including intramural) tumor growth, endoscopic surgery can be justified only as the first stage of treatment in the presence of complications or in weakened elderly patients in whom radical surgery poses an excessive risk.
Endoscopic surgery can be used as a palliative intervention for malignant tumors of the trachea and main bronchi in the following cases:
- For unresectable malignant tumors that cause obstruction of the trachea and large bronchi with symptoms of hypoxia, poststenotic infection, massive hemoptysis, indomitable cough. In this situation, endoscopic recanalization of the trachea or main bronchus followed by the introduction of a stent makes it possible to remove the patient from a critical condition, eliminate asphyxia and prolong the patient’s life, improving his quality of life, and also makes it possible to conduct a course of radiation or chemotherapy in safer conditions.
- For resectable malignant tumors of the main or lobar bronchi, when the severity of the patient’s condition, caused by severe ventilation disorders, post-stenotic pneumonia or suppuration in obstructed parts of the lung, does not allow radical surgery. In these cases, removal of the exophytic part of the tumor, restoring drainage and ventilation, makes it possible to reduce intoxication and hypoxia, improve the patient’s condition and prepare him for surgery.
- For resectable malignant tumors of large bronchi in elderly people or patients with severe somatic pathology, whose condition makes the risk of radical surgery extremely high, as well as in the case of the patient’s categorical refusal of radical surgery.
Indications for endoscopic surgical intervention are also granulation and cicatricial stenoses of the trachea and main bronchi that occur after tracheostomy or prolonged tracheal intubation, as well as (rarely) after resections and plastic surgeries on the trachea and large bronchi. Endoscopic surgery for this pathology is indicated in the following cases:
- In the presence of single granulations, often occurring in the trachea in the tracheostomy area or at the end of the tracheostomy cannula. In this case, laser evaporation can be quite successful and lead to recovery.
- For decompensated cicatricial stenosis of the trachea, accompanied by severe respiratory failure and/or purulent tracheobronchitis, making the risk of radical surgery excessively high. In most such cases, bronchoscopic recanalization of the trachea is performed on an emergency or emergency basis for health reasons and is a stage in preparing patients for circular resection of the stenotic section of the trachea.
- For decompensated cicatricial stenosis of the trachea in patients whose condition requires long-term treatment or rehabilitation and does not allow radical surgical intervention (patients with neurological consequences of severe traumatic brain injury, purulent complications of combined injuries or intracavitary surgical interventions, exhausted patients with aspiration pneumonia in combination stenoses with tracheoesophageal fistulas or defects).
- In case of decompensated or subcompensated cicatricial stenoses of the trachea of large extent (more than 8-9 cm), the presence of several stenoses or areas of tracheomalacia at different levels of the trachea, as well as recurrent stenoses after previous surgical interventions on the trachea, making its mobilization and resection almost impossible.
Bronchoscopic surgical interventions - these are real surgical operations, fraught with complications and adverse consequences.
Bleeding into the airway - one of the most real and dangerous complications. Bleeding more often occurs when highly vascularized benign and malignant tumors of the trachea and bronchi are removed.
The cause is usually mechanical damage to blood vessels tumors with a bronchoscope tube or instrument. But even when using an electrocoagulation loop and laser radiation, insufficient coagulation of blood vessels can be complicated by bleeding. Most dangerous bleeding when performing an operation under local anesthesia using a bronchofiberscope or videoscope. The blood instantly covers the lens, and visibility completely disappears, and through the narrow instrumental channel it is impossible to remove the intensely flowing blood and the clots that form. In this case, the patient can quickly lose consciousness and suffocate, “drowning” in his own blood. This circumstance forces most bronchologists to be critical of local anesthesia and flexible endoscopes when performing endoscopic interventions on the bronchi and to use them only in rare cases, for very narrow indications and in the presence of strong contraindications to general anesthesia. But even when performing a bronchoscopic operation under general anesthesia, the onset of even moderate-intensity bleeding significantly complicates the continuation of the intervention, impairing visibility and making it almost impossible to use the laser. Prevention of bleeding is careful coagulation of the tumor surface or area of stenosis before resection.
Unfortunately, predict in advance risk of bleeding This is not possible in all cases, so you should always be prepared for it: have a powerful electric suction, a supply of tuffers for pressing the bleeding site, a hemostatic gauze tape for tamponing the bronchus, hemostatic solutions (e-aminocaproic acid, transamcha, dicinone).
At bleeding , which we managed to cope with, we should not forget about the importance of thorough aspiration from the small bronchi of the blood spilled into them, for which, before extubation, it is necessary to perform a sanitation broncho-fibroscopy and bronchial lavage.
Perforation of the wall of the trachea or bronchus.
The occurrence of this complication is most real during laser recanalization of the trachea with its scar or tumor stenosis, as well as during evaporation of a tumor with predominantly endophytic growth that does not have clear boundaries. The wall of the trachea or bronchus can be burned , if you deviate from the axis of the lumen of the respiratory tube and go deeper into the tissue of the scar or tumor in the wrong direction. The most dangerous perforation of the wall is in those areas where the esophagus or large blood vessel is directly adjacent to the trachea or bronchus. A through wound in this location may be complicated by the development of a tracheoesophageal fistula or fatal bleeding. Therefore, it is not recommended to carry out deep evaporation of tumor tissue in the area of the membranous wall of the trachea or large bronchus or to capture the membranous wall of the trachea in a coagulation loop when removing the tumor emanating from it.” One must also be extremely careful when performing laser resection of tumors growing from the lateral wall of the left main bronchus or located in the spur area of the right main bronchus.
Strict adherence to the basic rules for the use of laser or electrosurgical equipment is the key to the safe performance of endoscopic operations.
The membranous wall of the trachea or main bronchus can be damaged by an attempt to bougienage cicatricial stenosis using a rigid bronchoscope tube without first cutting it with a laser, since it is the membranous wall of the trachea that is its weakest point. Even a small rupture of the wall of a large bronchus can be complicated by the development of mediastinal emphysema or pneumothorax, often tense.
This is facilitated by injection ventilation and coughing during the patient’s awakening and in the postoperative period. As a rule, subcutaneous emphysema occurs in the neck and anterior chest wall, identified by characteristic crepitus.
Penetrating wounds of the trachea and esophagus , as well as damage to the walls of the respiratory tract, accompanied by increasing emphysema of the mediastinum, require emergency thoracotomy and suturing of the defect. Along with this, limited defects in the tracheal wall without damage to the esophagus can heal on their own if they are temporarily closed with an endotracheal stent and large doses of antibiotics are prescribed, as we have repeatedly had the opportunity to verify.
Ignition of the light guide in the lumen of the respiratory tract can have very serious consequences. This can happen if you use fibers without air or gas cooling.
During bronchoscopy under general anesthesia with mechanical ventilation, an increased concentration of oxygen is created in the lumen of the trachea and bronchi. In an oxygen-saturated atmosphere, the synthetic fiber sheath can ignite, causing severe burns to the mucous membrane of the respiratory tract. This can also happen if the laser beam hits an object made of flammable material inserted into the trachea: endotracheal tube, tracheotomy cannula, endotracheal stent, catheter for injection ventilation, foreign body of organic origin.
Here is an observation.
Patient G., 26 years old, resident of North Ossetia, during a feast, choked on a piece of meat and began to choke. One of the friends tried to push a piece stuck in the laryngopharynx into the esophagus with the help of the first wooden sliver that came to hand. The patient managed to swallow the meat, but after this he developed a constant cough, and after 2 weeks wheezing began.
Laryngoscopy revealed thickening of the wall and narrowing of the tracheal lumen in the subglottic space, and therefore the patient was sent to the All-Russian Oncological Research Center (ONRC) named after. N. N. Blokhin RAMS. The pathology was assessed as a tracheal tumor, and it was decided to perform laser resection. During the evaporation of the “tumor”, performed under general anesthesia with mechanical ventilation with oxygen, a fragment of a wooden chip ignited, stuck into the wall of the trachea directly under the ligaments and caused a pronounced proliferative reaction, mistaken for a tumor. A severe burn of the tracheal mucosa followed, causing the development of several cicatricial stenoses throughout the trachea, the most significant of which, about 5 cm in length, was localized in the lower half of the thoracic part of the trachea.
For further treatment in November 1997, the patient was transferred to our clinic with severe stridor breathing and respiratory failure. Laser recanalization of the trachea was performed, a 6 cm long endotracheal Dumont stent was installed in the area of the lower stricture, after which the patient was discharged in satisfactory condition. Circular tracheal resection was considered impracticable due to the multiple nature of the strictures and the extent of the tracheal lesion. Over the next 3 years, the patient was hospitalized three times to replace the endoprosthesis and remove granulations (Fig. 1). The length of the stenoses increased each time. The possibility of installing a bifurcation dynamic Freitag stent was discussed. In September 2000, due to another deterioration in breathing and expectoration, the patient intended to come to the clinic, but in early October he suddenly developed an attack of suffocation, which led to death.
To prevent such complications, it is necessary to cool the end of the light guide with air. or compressed inert gas. For this we use a conventional compressor, and in recent years - carbon dioxide, a cylinder with which is installed in the bronchoscopy room. Gas under a pressure of 1 - 1.5 is injected into the plastic cover of the light guide at its proximal end. Thanks to this, having performed a large number of laser operations under conditions of general anesthesia with oxygen injection ventilation, we avoided ignition of the light guide in the lumen of the respiratory tract. The only case occurred during testing of a holmium YAG laser, the optical fibers of which were not equipped with a gas cooling system. Therefore, as our experience shows, if the fiber sheath is adequately purged, the risk of its ignition is low, even when the operation is performed under general anesthesia with mechanical ventilation.
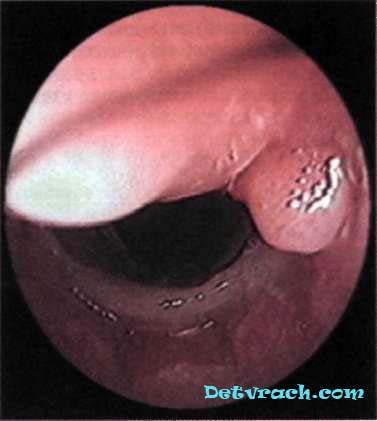
Rice. 1. Bronchoscopy of patient G., 26 years old, with cicatricial stenosis of the trachea after a thermal burn. Granulations at the proximal end of the endotracheal stent.
However, we consider it advisable to turn on laser radiation only against the background of apnea, which reduces the oxygen concentration in the lumen of the respiratory tract at the time of evaporation and also makes the object motionless. In addition, we categorically do not recommend using laser radiation if there are tubes, stents, catheters, etc. in the lumen of the respiratory tract, for example, removing granulations at the ends of the stent with a laser.
Gas or air passing inside the fiber sheath blows smoke and charred tissue particles from the end. This improves visibility during surgery and reduces the burning of the ends of the light guides. It should be noted that the use of carbon dioxide to cool light guides when performing bronchofibroscopy under local anesthesia causes uncontrollable coughing in patients. In such cases, the only option is to blow the light guides with atmospheric air using a compressor.
Another complication is associated with the use of a bronchial fiberscope as a conductor for a laser light guide. When the distal end of the bronchofiberscope was significantly bent along with the light guide passed through its channel during laser evaporation of a tumor of the upper lobe bronchus, the light guide shell suddenly burned through in the area of maximum bending and the tube of the bronchofiberscope was so badly damaged that it required its complete replacement. Since then, we have tried to use bronchofiberscopes as little as possible during laser operations and carefully monitor the degree of bending of the light guide.
Anesthetic complications arising during bronchoscopic surgical interventions, are not much different from those during diagnostic and therapeutic bronchoscopy and were described in detail by us earlier.
It should be noted once again that endoscopic operations on the trachea, as a rule, are accompanied by more significant trauma and require the addition of local anesthesia in the operated area. Without this, the frequency of laryngospasm and painful cough increases when the patient awakens and in the postoperative period.