Subcutaneous injections are in high demand medical procedure. The technique for performing it differs from the technique for introducing medicines intramuscularly, although the preparation algorithm is similar.
The injection should be made subcutaneously less deeply: it is enough to insert the needle inside just 15 mm. Subcutaneous tissue has a good blood supply, which determines high speed absorption and, accordingly, the action of drugs. Just 30 minutes after injection medicinal solution observed maximum effect from his action.

The most convenient places for administering drugs subcutaneously:
- shoulder (its outer region or middle third);
- anterior outer surface of the thighs;
- lateral part of the abdominal wall;
- subscapular region in the presence of pronounced subcutaneous fat.
Preparatory stage
Execution algorithm of any medical manipulation, as a result of which the integrity of the patient’s tissues is compromised, begins with preparation. Before giving the injection, you should disinfect your hands: wash them antibacterial soap or treat with an antiseptic.
Important: For protection purposes own health The standard algorithm for the work of medical personnel during any type of contact with patients involves wearing sterile gloves.
Preparation of instruments and preparations:
- a sterile tray (a clean ceramic plate that has been disinfected by wiping) and a tray for waste materials;
- a syringe with a volume of 1 or 2 ml with a needle with a length of 2 to 3 cm and a diameter of no more than 0.5 mm;
- sterile wipes (cotton swabs) – 4 pcs.;
- prescribed drug;
- alcohol 70%.
Everything that will be used during the procedure should be on a sterile tray. You should check the expiration date and tightness of the packaging of the medicine and the syringe.
The place where you plan to give the injection must be inspected for the presence of:
- mechanical damage;
- swelling;
- signs of dermatological diseases;
- manifestation of allergies.
If the selected area has the problems described above, the location of the intervention should be changed.
Taking medicine
The algorithm for withdrawing the prescribed drug into a syringe is standard:
- checking the compliance of the medicine contained in the ampoule with that prescribed by the doctor;
- clarification of dosage;
- disinfection of the neck at the point of its transition from the wide part to the narrow part and incision with a special file supplied in the same box with the medicine. Sometimes ampoules have specially weakened places for opening, made in a factory way. Then there will be a mark on the vessel in the indicated area - a colored horizontal stripe. The removed top of the ampoule is placed in a waste tray;
- the ampoule is opened by wrapping the neck with a sterile swab and breaking it away from you;
- the syringe is opened, its cannula is combined with the needle, and then the case is removed from it;
- the needle is placed in the opened ampoule;
- the syringe plunger is retracted thumb, fluid is taken;
- the syringe rises with the needle up; the cylinder should be lightly tapped with your finger to displace the air. Push the medicine with the plunger until a drop appears at the tip of the needle;
- attach the needle case.
Before you do subcutaneous injections it is necessary to disinfect the surgical field (side, shoulder): with one (large) swab soaked in alcohol, a large surface is treated, with the second (middle) the place where the injection is directly planned to be given. Technique for sterilizing the work area: moving the swab centrifugally or from top to bottom. The injection site should be dry from alcohol.

Manipulation algorithm:
- the syringe is taken in the right hand. The index finger is placed on the cannula, the little finger is placed on the piston, the rest will be on the cylinder;
- left hand - big and index fingers– grab the skin. There should be a skin fold;
- to make an injection, the needle is inserted with a cut upward at an angle of 40-45º for 2/3 of the length into the base of the resulting skin fold;
- forefinger right hand maintains its position on the cannula, and left hand transfers to the piston and begins to press it, slowly injecting the medicine;
- a swab soaked in alcohol is easily pressed against the insertion site of the needle, which can now be removed. Safety precautions stipulate that during the process of removing the tip, you should hold the place where the needle is attached to the syringe;
- after finishing the injection, the patient should hold the cotton ball for another 5 minutes, the used syringe is separated from the needle. The syringe is thrown away, the cannula and needle break.
Important: Before giving the injection, the patient must be positioned comfortably. During the injection process, it is necessary to continuously monitor the person’s condition and his reaction to the intervention. Sometimes it is better to give the injection while the patient is lying down.
When you finish giving the injection, take off your gloves if you were wearing them and disinfect your hands again: wash or wipe with an antiseptic.

If you completely follow the algorithm for performing this manipulation, then the risk of infections, infiltrates and other negative consequences decreases sharply.
Oil solutions
Do intravenous injections oil solutions are prohibited: such substances clog blood vessels, disrupting the nutrition of adjacent tissues, causing their necrosis. Oil emboli may well end up in the vessels of the lungs, blocking them, which will lead to severe suffocation, followed by death.
Oily preparations are poorly absorbed, so infiltrates are common at the injection site.
Tip: To prevent infiltration, you can put a heating pad (make a warm compress) at the injection site.
Introduction algorithm oil solution provides for preliminary heating of the drug to 38ºС. Before making an injection and administering the medicine, you should insert the needle under the patient’s skin, pull the syringe plunger towards you and make sure that it has not been damaged blood vessel. If blood enters the cylinder, lightly press the needle insertion site with a sterile swab, remove the needle and try again in another place. In this case, safety precautions require replacing the needle, because used is no longer sterile.
 How to inject yourself: rules of procedure
How to inject yourself: rules of procedure
 Where to give an injection in the buttock correctly - diagram and instructions
Where to give an injection in the buttock correctly - diagram and instructions
 Injection in the leg at home - how to do it correctly?
Injection in the leg at home - how to do it correctly?
ATX code: G03GA05
RFH: Recombinant human follicle-stimulating hormone
ICD-10 codes (indications): E23.0, N97, Z31.1
KFU code: 15.06.05.01
Manufacturer: MERCK SERONO S.p.A. (Italy)
DOSAGE FORM, COMPOSITION AND PACKAGING
Solution for subcutaneous administration
Excipients:
0.5 ml - syringe pens (1) complete with disposable needles (5 pcs.) - plastic containers (1) - cardboard boxes.
Solution for subcutaneous administration transparent, colorless, slight opalescence is allowed.
Excipients: poloxamer 188, sucrose, methionine, sodium dihydrogen phosphate monohydrate, sodium hydrogen phosphate dihydrate, m-cresol, phosphoric acid, sodium hydroxide, water d/i.
0.75 ml - syringe pens (1) complete with disposable needles (7 pcs.) - plastic containers (1) - cardboard boxes.
Solution for subcutaneous administration transparent, colorless, slight opalescence is allowed.
Excipients: poloxamer 188, sucrose, methionine, sodium dihydrogen phosphate monohydrate, sodium hydrogen phosphate dihydrate, m-cresol, phosphoric acid, sodium hydroxide, water d/i.
1.5 ml - syringe pens (1) complete with disposable needles (14 pcs.) - plastic containers (1) - cardboard boxes.
PHARMACHOLOGIC EFFECT
Recombinant human follicle stimulating hormone. The drug is obtained by the method genetic engineering on a culture of Chinese hamster ovary cells. Has a gonadotropic effect: stimulates the growth and maturation of the follicle/follicles, promotes the development of several follicles during controlled ovarian hyperstimulation for assisted reproductive technology programs.
PHARMACOKINETICS
Suction
With subcutaneous administration, the absolute bioavailability is approximately 70%.
In women with suppressed secretion of endogenous gonadotropins, follitropin alfa has been shown to effectively stimulate follicular development and steroidogenesis, despite low measurable LH levels.
Distribution and elimination
After repeated injections of the drug Gonal-F ® there is a threefold accumulation of the drug in the blood compared to a single injection. C ss in the blood is achieved within 3-4 days. V d is 10 l.
After intravenous administration, follitropin alpha is detected in the extracellular fluid. The initial T1/2 from the body is approximately 2 hours, the final T1/2 is approximately 24 hours.
1/8 of the administered dose of follitropin alfa is excreted in the urine. Total clearance - 0.6 l/h.
INDICATIONS
Women
Ovarian stimulation in the absence of growth and maturation of follicles (including with polycystic ovary syndrome) and in case of ineffectiveness of therapy with clomiphene citrate;
Controlled ovarian hyperstimulation in assisted reproductive technology programs;
Ovarian stimulation in hypogonadotropic conditions in women (in combination with LH).
Men
Stimulation of spermatogenesis in hypogonadotropic hypogonadism in men (in combination with human chorionic gonadotropin).
DOSING REGIME
The drug is administered subcutaneously.
Women
At anovulatory infertility with a preserved menstrual cycle or with a violation of its periodicity Treatment begins in the first 7 days of the cycle. Stimulation is carried out under ultrasound control (follicle sizes are measured) and/or estrogen levels. Stimulation begins with a daily dose of 75-150 ME, increasing it by 37.5 ME-75 ME after 7-14 days until the desired effect is obtained. The maximum dose for one injection is 225 IU. If there is no positive dynamics after 4 weeks, treatment is stopped. IN next cycle stimulation should be started with a higher dose.
After reaching optimal sizes follicles 24-48 hours after the last injection of the drug Gonal-F ® a single dose of recombinant human chorionic gonadotropin (hCG) is administered at a dose of 250 mcg or hCG at a dose of 5000-10,000 IU. On the day of hCG injection and the next day, the patient is recommended to have sexual intercourse.
In case of excessive ovarian response to stimulation, the administration of human chorionic gonadotropin should be discontinued. In the next cycle, a lower dose is prescribed compared to the previous one.
At conducting controlled ovarian hyperstimulation for assisted reproductive technologies Gonal-F ® is prescribed daily at a dose of 150-225 IU, starting from the 2-3rd day of the cycle. The daily dose may vary, but usually does not exceed 450 IU. Treatment is continued until the follicles reach adequate size according to ultrasound (on average 5-20 days). 24-48 hours after the last injection of the drug Gonal-F ® a single dose of recombinant hCG is administered at a dose of 250 mcg or hCG at a dose of 5000-10,000 IU to induce the final maturation of follicles.
GnRH analogues are used to suppress the endogenous LH surge and maintain it at a low level.
At anovulatory infertility with absence menstrual cycle as a result of FSH and LH deficiency The doctor determines the dose of the drug and treatment regimen individually. Typically, Gonal-F ® is prescribed daily for up to 5 weeks concomitantly with LH. Treatment with Gonal-F ® begins with a dose of 75-150 IU simultaneously with lutropin alfa at a dose of 75 IU. If necessary, the dose of Gonal-F ® can be increased by 37.5-75 IU every 7-14 days. If there is no adequate response to stimulation within 5 weeks, therapy should be stopped and resumed in a new cycle at a higher dose.
After reaching the optimal size of the follicle/follicles, 24-48 hours after the last injection of the drug Gonal-F ® and lutropin alfa, a single dose of recombinant hCG is administered at a dose of 250 mcg or hCG at a dose of 5000-10,000 IU. On the day of hCG injection and the next day, the patient is recommended to have sexual intercourse. As an alternative, intrauterine insemination may be performed.
If the ovaries respond excessively to stimulation, treatment should be discontinued and hCG should be discontinued. Stimulation is repeated in the next cycle, starting with a lower dose compared to the previous cycle.
Men
Gonal-F ® is prescribed, as a rule, at a dose of 150 IU 3 times a week for at least 4 months in combination with hCG. With absence positive effect During this time, treatment can be continued for up to 18 months.
Rules for administering the drug
When using the drug independently, patients should carefully study the instructions.
The packaging of the drug is intended for individual use. After the first injection, the next injection should be given the next day at the same time.
1. The injection should be carried out in compliance with the rules of asepsis and antisepsis.
2. To carry out the injection, you need to lay out 2 alcohol-soaked swabs, a pre-filled syringe pen and an injection needle on a clean surface.
Preparing a pre-filled syringe pen of the drug Gonal-F ® for the first use: remove the cap of the pen, put on the needle as described in step 3. Then fill the syringe pen by placing the dose indicator arrow opposite point 37.5 on the black disk to set the dose. Press the injection button all the way, remove the outer needle cap, then the inner needle cap, while holding the syringe pen with the needle vertically (the needle should be pointing up). Gently tap the cartridge location so that any air bubbles collect at the base of the needle. While pointing the needle vertically upward, release the injection button completely. A drop may appear at the tip of the needle. This means the pre-filled pen is ready to be injected. A loss small amount the liquid at the tip of the needle does not matter, because the syringe pen is specially filled with some excess. If liquid does not appear at the tip of the needle, then the preparation process should be repeated. Then the dose should be set as described in paragraph 4.
For the next injection, attach the needle and set the dose as described in paragraphs. 3 and 4 respectively.
3. Attaching the needle. Get a new needle. If the needle packaging is broken, you should throw the needle away and get a new one. Remove the protective label from the outer needle cap, remove the protective label from the inner needle cap. Holding the needle firmly by the inner cap, insert the threaded tip into the needle and turn clockwise until it clicks into place. Only use the needles included with the pen or supplied separately for this pen.
4. Dose setting. Set the required dose by turning the dose setting dial until the dose value is opposite the arrow. The dose dial allows you to set the dose in 37.5 IU intervals. Minimum dose and maximum dose are in the range from 37.5 ME to 300 ME. After establishing the required dose, dial it by pressing the injection button all the way. It is necessary to carefully monitor the set dose on the disk, because Once the injection button is pressed, it can no longer be changed. If, after pressing the injection button and dialing the dose, it turns out that the dose was dialed incorrectly, then the injection should not be given. Delete the erroneously dialed dose and repeat the dialing again. The red dose control dial should be checked to ensure that correct dose: When the injection button is released, the number on the red control dial indicating the dose dialed is opposite the dose set on the black dial dial against the arrow. If the dialed dose is less than the required one, then dosing is not completed. In this case, you must act in accordance with clause 2.
If the same dose is required each time, the dose indicator arrow should remain in the same position.
5. The injection site chosen on the doctor’s recommendation should be treated with an alcohol swab. Insert the needle into the skin and press the injection button. Leave the needle in the skin for at least 10 seconds. Keep the button pressed as long as the needle remains in the skin. This ensures that the required dose is completely administered.
6. Removing the needle. The needle should be thrown away after each injection. Holding the syringe pen firmly by the drug reservoir, carefully place the outer cap on the needle. Clamp the outer needle cap and unscrew the needle by turning it counterclockwise. Throw away the used needle. Place the protective cap on the syringe pen.
7. Storing a pre-filled pen. After injection, remove used needles as described in step 6. Place the protective cap on the syringe pen. The syringe pen should be stored in safe place, preferably in original packaging. Once the pen is empty, you should throw it away.
Note: The scale that can be seen through the drug reservoir serves as an indicator of the amount of drug remaining in the reservoir. It cannot be used to set the dose. The red dose control dial on the injection button monitors whether the last dose has been fully injected. It changes its position, indicating the amount of drug in the reservoir. If the collected dose is not sufficient to complete the injection, there are two options: a) inject the dose remaining in the pen, and then take a new pen, set the remainder of the required dose on it and inject it; b) throw away the old syringe pen, take a new one and administer the required dose.
Patients should be warned to seek medical attention if injected high dose than required, or in case of missing the next dose; Do not administer a double dose of the drug.
SIDE EFFECT
Frequency determination side effects: very often (>1/10,<1/100), часто (>1/100, < 1/1000), редко (>1/10 000, <1/1000), очень редко (< 1/10 000).
Women
very often - ovarian cysts; often - ovarian hyperstimulation syndrome (OHSS) of mild or moderate severity; rarely - severe form of OHSS, torsion of an ovarian cyst (as a complication of OHSS), ovarian apoplexy, ectopic pregnancy (if a history indicates diseases of the fallopian tubes), multiple pregnancy. A mild form of OHSS is accompanied by pain in the lower abdomen, nausea, vomiting, weight gain, enlarged ovaries, incl. due to the formation of cysts. In moderate and severe forms of OHSS, in addition, shortness of breath, oliguria, ascites, hydrothorax, pleural effusion, and fluid accumulation in the pericardial cavity are noted; Acute pulmonary failure and thromboembolism are possible.
From the side of the central nervous system: often - headache.
From the digestive system: often - abdominal pain, nausea, vomiting, diarrhea, colic, belching.
From the cardiovascular system: very rarely - increased blood clotting (thromboembolism), pulmonary embolism, ischemic stroke, myocardial infarction.
From the respiratory system: very rarely - in patients with bronchial asthma, worsening or exacerbation of the disease.
Allergic reactions: very rarely - mild systemic allergic reactions (redness of the skin, rash, swelling of the face, urticaria, difficulty breathing), severe allergic reactions (including anaphylaxis).
Other: fever, arthralgia.
Local reactions:
Men
From the endocrine system: often - gynecomastia, varicocele.
Dermatological reactions: often - the appearance of acne (acne).
Other: often - weight gain.
Local reactions: very often - mild or moderate pain, redness, bruising, swelling at the injection site.
CONTRAINDICATIONS
Hypothalamic-pituitary tumors;
Hypersensitivity to the components of the drug.
Women
Pregnancy;
Volumetric neoplasms or ovarian cysts (not caused by polycystic ovary syndrome);
Uterine bleeding of unknown etiology;
Ovarian carcinoma;
Uterine cancer;
Breast cancer;
Anomalies in the development of the genital organs and uterine fibroids, incompatible with pregnancy;
Primary ovarian failure;
Premature menopause.
Men
Primary testicular failure.
PREGNANCY AND LACTATION
The drug is not prescribed during pregnancy and lactation.
SPECIAL INSTRUCTIONS
Because Gonal-F ® can cause serious adverse reactions and should only be prescribed by a specialist doctor directly involved in infertility problems. The start of therapy should be preceded by an examination of the infertile couple, in particular, studies should be carried out to exclude hypothyroidism, adrenal insufficiency, hyperprolactinemia, hypothalamic-pituitary tumors, and, if necessary, appropriate therapy should be prescribed.
It is necessary to assess the patency of the fallopian tubes in order to select a method of assisted reproductive technology. Fallopian tube obstruction should be excluded if the patient is not participating in an in vitro fertilization program. In patients with porphyria, as well as in the presence of porphyria in relatives, careful monitoring is required during therapy with Gonal-F ®. If the condition worsens or the first signs of this disease appear, it may be necessary to discontinue therapy. When treating with the drug, it is necessary to assess the condition of the ovaries using ultrasound, both separately and in combination with the determination of estradiol in the blood plasma. The drug should be used in the minimum effective dose in both women and men.
When hCG is prescribed, the likelihood of OHSS and multiple superovulation increases. Therefore, if the ovaries have an excessive response to hCG stimulation, hCG is not prescribed, and patients are advised to abstain from coitus for at least 4 days or use barrier methods of contraception. The likelihood of OHSS in patients undergoing controlled ovarian hyperstimulation in assisted reproductive technology programs is reduced by aspiration of all follicles.
The degree of risk of multiple pregnancy with assisted reproductive technologies depends on the number of embryos transferred; twin pregnancies are more common. After ovulation induction, the incidence of multiple pregnancies and births increases compared to natural conception.
The frequency of pregnancy terminations after ovulation induction and assisted reproductive technology programs is slightly higher than in the population, but comparable to the rates for women suffering from other forms of infertility.
The likelihood of an ectopic pregnancy after assisted reproductive technology programs is 2% to 5%, compared to 1-1.5% in the general population.
A high level of FSH in the blood serum of men may indicate primary testicular failure. In this case, treatment with Gonal-F ® is ineffective.
To assess the response to Gonal-F ® stimulation, it is recommended to monitor spermograms 4-6 months after the start of therapy.
It is necessary to obtain information about all types of allergic reactions that patients have, as well as about all drugs that patients received before starting treatment with Gonal-F ® .
Patients should be warned to notify their physician if they experience any serious side effects or effects not described above.
It is necessary to mark the date of the first day of use on the pen with the drug. Do not use the drug solution after 28 days from the date of first use. The drug can be stored for 28 days at room temperature not higher than 25°C. The drug should be destroyed if it is not used during this period.
Impact on the ability to drive vehicles and operate machinery
Gonal-F ® does not affect the ability to drive vehicles or operate machinery.
OVERDOSE
Currently, no cases of overdose of the drug Gonal-F ® have been reported. When using the drug in excessive doses, the development of OHSS should apparently be expected.
DRUG INTERACTIONS
When Gonal-F ® is combined with other stimulating drugs (hCG, clomiphene citrate), the ovarian response is enhanced; against the background of desensitization of the pituitary gland with GnRH analogues, it decreases (an increase in the dose of the drug is required).
There is no data on the incompatibility of the drug Gonal-F ® with other drugs.
CONDITIONS OF VACATION FROM PHARMACIES
The drug is available with a prescription.
CONDITIONS AND DURATION OF STORAGE
The drug should be stored out of the reach of children, protected from light, in its original packaging at a temperature of 2° to 8°C; do not freeze. Shelf life - 2 years.
The subcutaneous fat layer is well supplied with blood vessels, therefore, for faster action of the drug, subcutaneous injections (SC) are used. Drugs administered subcutaneously are absorbed more quickly than when administered orally. Subcutaneous injections are made with a needle to a depth of 15 mm and up to 2 ml of medications are injected, which are quickly absorbed into the loose subcutaneous tissue and do not have a harmful effect on it.
Characteristics of needles and syringes for subcutaneous injections :
Needle length -20 mm
Section -0.4 mm
Syringe volume - 1; 2 ml Subcutaneous injection sites:
The middle third of the anterior outer surface of the shoulder;
The middle third of the anterior outer surface of the thigh;
Subscapular region;
Anterior abdominal wall.
In these places, the skin is easily caught in the fold and there is no danger of damage to blood vessels, nerves and periosteum. It is not recommended to inject: into places with edematous subcutaneous fat; in compactions from poorly absorbed previous injections.
Equipment:
Execution algorithm:
Put on a clean gown, a mask, sanitize your hands, and put on gloves.
Draw up the medicine, release the air from the syringe, and place it in the tray.
Have the patient sit or lie down, depending on the choice of injection site and drug.
Inspect and palpate the injection area.
Treat the injection site sequentially in one direction with 2 cotton balls moistened with a 70% alcohol solution: first a large area, then the second ball directly at the injection site, place it under the little finger of your left hand.
Take the syringe in your right hand (hold the needle cannula with the index finger of your right hand, hold the syringe plunger with your little finger, hold the cylinder with fingers 1, 3, 4).
With your left hand, gather the skin into a triangular fold, base down.
Insert the needle at an angle of 45° with the cut up into the base of the skin fold to a depth of 1-2 cm (2/3 of the needle length), hold the needle cannula with your index finger.
Place your left hand on the plunger and inject the medication (do not transfer the syringe from one hand to the other).
Remove gloves and place in
Wash hands, dry.
Note. During the injection and after it, 15-30 minutes later, ask the patient about his well-being and reaction to the injected drug (identifying complications and reactions).
Fig. 1.Sites for subcutaneous injections
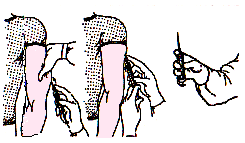
Fig.2. SC injection technique.
Subcutaneous injection of oil solutions.
Target: medicinal.
Indications: administration of hormonal drugs, solutions of fat-soluble vitamin preparations.
Equipment:
Sterile: a tray with gauze pads or cotton balls, a syringe with a volume of 1.0 or 2.0 ml, 2 needles, 70% alcohol, drugs, gloves.
Non-sterile: scissors, couch or chair, containers for disinfecting needles, syringes, dressings.
Execution algorithm:
Explain the procedure to the patient and obtain his consent.
Put on a clean gown, mask, sanitize your hands, and put on gloves.
Before use, immerse the ampoule in a container with warm water and heat it to 38°C.
Fill the syringe with the medicine and release the air from the syringe.
Treat the injection site twice with tufikomi with 70% alcohol.
Inject with a needle, pull the plunger towards you - make sure that no blood enters the syringe - preventing drug embolism (oil embolism).
Slowly introduce the solution (temperature of the oil solution is 38°C).
Apply pressure to the injection site with a cotton ball containing 70% alcohol.
Remove the needle by holding it by the cannula.
Place the disposable syringe and needle in a container with 3% chloramine for 60 minutes.
Remove gloves, place a container with a disinfectant solution.
Wash hands, dry.
Lyophilisate for the preparation of a solution for subcutaneous administration, almost white in color, dispersible in the supplied solvent to form a clear solution, practically free of particles. 1 fl. triptorelin (in acetate form) 100 mcg. Excipients: mannitol 10 mg. Solvent: sodium chloride solution 0.9% - 1 ml.
Clinical and pharmacological group: Gonadotropin-releasing hormone analogue.
pharmachologic effect
Synthetic decapeptide, analogue of natural GnRH. Diferelin, after an initial period of stimulation, with long-term use suppresses the secretion of gonadotropin with subsequent inhibition of ovarian function. Constant use of Diferelin suppresses the secretion of gonadotropin (FSH and LH). Suppression of intermediate endogenous LH peaks makes it possible to improve the quality of folliculogenesis, while at the same time the number of maturing follicles increases, and as a result, the likelihood of pregnancy per cycle increases.
Pharmacokinetics
Suction
After subcutaneous administration of Diferelin at a dose of 100 mcg, triptorelin is rapidly absorbed. Cmax in blood plasma is reached after 0.63±0.26 hours and is 1.85±0.23 ng/ml.
Distribution
The distribution phase ends after 3-4 hours, Vd is 1562±158 ml/kg.
Removal
T1/2 is 7.6±1.6 hours. Total plasma clearance is 161±28 ml/min.
Indications
female infertility, ovarian stimulation together with gonadotropins (hMG, hCG, FSH) in in vitro fertilization and embryo transfer programs, as well as other assisted reproductive technologies.
Dosage regimen
Short course of treatment Diferelin is administered subcutaneously at a dose of 100 mcg/day every day, starting from the 2nd day of the cycle (at the same time starting ovarian stimulation), and treatment is completed 1 day before the planned administration of human chorionic gonadotropin. The course of treatment is 10-12 days. Long-term treatment Diferelin is administered subcutaneously at a dose of 100 mcg/day every day, starting from the 2nd day of the cycle.
When the pituitary gland is desensitized (E2 less than 50 pg/ml, i.e. approximately on the 15th day after the start of treatment), stimulation of the ovaries with gonadotropins begins and subcutaneous injections of Diferelin are continued at a dose of 100 mcg/day, ending them 1 day before planned administration of human chorionic gonadotropin. The duration of treatment is determined by the doctor individually.
Rules for preparing the solution
The supplied solvent is added to the vial with the lyophilisate and shaken until completely dissolved.
Used needles should be placed in a sharps container.
Side effect
At the beginning of treatment
From the reproductive system: when combined with gonadotropins, ovarian hyperstimulation is possible (increase in ovarian size, abdominal pain).
During treatment
From the reproductive system: most often - sudden hot flashes, vaginal dryness, decreased libido and dyspareunia associated with pituitary-ovarian blockade.
From the digestive system: not often - nausea, vomiting, weight gain.
From the central nervous system and peripheral nervous system: not often - emotional lability, visual impairment; in some cases - headache.
From the musculoskeletal system: possible bone demineralization, increased risk of osteoporosis (with long-term use of the product); in some cases - arthralgia, myalgia.
From the cardiovascular system: not often - increased blood pressure.
Allergic reactions: urticaria, skin rash, itching; not often - Quincke's edema.
Local reactions: uncommon - pain at the site of administration of the product.
Contraindications
pregnancy;
high sensitivity to product components.
Pregnancy and lactation
Diferelin is contraindicated for use during pregnancy. However, practice has shown that after ovulation stimulated in the previous cycle, in some cases pregnancy occurred without stimulation, and the further course of ovulation stimulation continued. Two well-performed experimental studies on animals did not reveal the teratogenic effects of Diferelin.
Therefore, the development of congenital anomalies in humans is not expected when using the product. The results of clinical studies involving a small number of pregnant women who received a GnRH analogue showed the absence of fetal malformations or fetotoxicity.
However, further study is needed into the effects of the product on pregnancy.
special instructions
The response of the ovaries to subcutaneous administration of Diferelin in combination with gonadotropins can markedly increase in predisposed patients, in particular in the case of polycystic ovary syndrome. The response of the ovaries to the administration of the product in combination with gonadotropins may vary among patients; in addition, the reaction may be different in the same patients during different cycles.
Stimulation of ovulation should be carried out under the supervision of a physician and regular analysis using biological and clinical methods: increasing the content of estrogen in plasma and ultrasound echography. If the ovarian response is excessive, it is recommended to interrupt the stimulation cycle and stop gonadotropin injections.
Impact on the ability to drive vehicles and operate machinery
The drug does not affect the ability to drive vehicles or operate machinery.
Overdose
There are no known cases of overdose of Diferelin.
Drug interactions
Drug interactions with Diferelin have not been described.
Storage conditions and periods
The drug should be stored out of reach of children at a temperature not exceeding 25°C. Shelf life - 2 years.
Attention!Before using the medication "Diphereline for subcutaneous administration" You should consult your doctor.
The instructions are provided for informational purposes only. Diphereline for subcutaneous administration».
The subcutaneous fat layer is well supplied with blood vessels, therefore, for faster action of the drug, subcutaneous injections (SC) are used. Drugs administered subcutaneously are absorbed more quickly than when administered orally. Subcutaneous injections are made with a needle to a depth of 15 mm and up to 2 ml of medications are injected, which are quickly absorbed into the loose subcutaneous tissue and do not have a harmful effect on it.
Characteristics of needles and syringes for subcutaneous injections:
Needle length -20 mm
Section -0.4 mm
Syringe volume - 1; 2 ml
Subcutaneous injection sites:
The middle third of the anterior outer surface of the shoulder;
The middle third of the anterior outer surface of the thigh;
Subscapular region;
Anterior abdominal wall.
In these places, the skin is easily caught in the fold and there is no danger of damage to blood vessels, nerves and periosteum. It is not recommended to inject: into places with edematous subcutaneous fat; in compactions from poorly absorbed previous injections.
Equipment:
Sterile: a tray with gauze pads or cotton balls, a syringe with a volume of 1.0 or 2.0 ml, 2 needles, 70% alcohol, drugs, gloves.
Non-sterile: scissors, couch or chair, containers for disinfecting needles, syringes, dressings.
Execution algorithm:
1. Explain the procedure to the patient and obtain his consent.
2. Put on a clean gown, mask, sanitize your hands, and put on gloves.
3. Draw up the medicine, release the air from the syringe, and place it in the tray.
4. Sit or lie down the patient, depending on the choice of injection site and drug.
5. Inspect and palpate the injection area.
6. Treat the injection site sequentially in one direction with 2 cotton balls moistened with a 70% alcohol solution: first a large area, then the second ball directly at the injection site, place it under the little finger of your left hand.
7. Take the syringe in your right hand (hold the needle cannula with the index finger of your right hand, hold the syringe plunger with your little finger, hold the cylinder with fingers 1,3,4).
8. With your left hand, gather the skin into a triangular fold, base down.
9. Insert the needle at an angle of 45° with the cut upward into the base of the skin fold to a depth of 1-2 cm (2/3 of the needle length), hold the needle cannula with your index finger.
10. Place your left hand on the plunger and inject the medication (do not transfer the syringe from one hand to the other).
11. Press the injection site with a cotton ball with 70% alcohol.
12. Remove the needle by holding it by the cannula.
13. Place the disposable syringe and needle in a container with 3% chloramine for 60 minutes.
14. Remove gloves and place in a container with a disinfectant solution.
15. Wash hands and dry.
Note. During the injection and after it, 15-30 minutes later, ask the patient about his well-being and reaction to the injected drug (identifying complications and reactions).
Fig. 1.Sites for subcutaneous injections

Fig.2. SC injection technique.